Level of severity
94% of akathisia events were mild or moderate in patients treated with VRAYLAR + ADT in the two 6-week MDD studies
| Mean change at endpoint | Proportion of patients with weight increase ≥7% | |
|---|---|---|
| Placebo + ADT (n=503) | +0.4 lb | 1% |
| VRAYLAR 1.5 mg/day + ADT (n=502) | +1.5 lb | 2% |
| VRAYLAR 3 mg/day + ADT (n=503) | +1.5 lb | 2% |
In 6-week MDD studies, VRAYLAR demonstrated metabolic shifts similar to placebo for total cholesterol and fasting triglycerides when taken with an antidepressant1,2
| Total cholesterol | Proportion of patients with metabolic shifts was similar to placebo† |
|---|---|
| Fasting triglycerides | |
| Fasting glucose | 97% of patients did not have a clinically meaningful increase in blood glucose‡ |
| Prolactin (ng/mL)§ | No meaningful increase in mean levels |
(See bipolar I depression tab above)
*In the 8-week MDD study, 2.5% of people taking VRAYLAR + ADT had a weight increase of ≥7% vs 2% of those taking placebo. The mean weight changes reported in this study were VRAYLAR 1-2 mg/day + ADT (n=273) = +1.98 lb; VRAYLAR 2-4.5 mg/day + ADT (n=273) = +1.98 lb; placebo + ADT (n=266) = 0 lb.1 See additional weight data from 26-week MDD study.
†In the 6- and 8-week MDD studies, proportion of patients with metabolic shifts was similar to placebo. Shift defined as: total cholesterol: normal/borderline (<240 mg/dL) to high (≥240 mg/dL); fasting triglycerides: normal/borderline (<200 mg/dL) to high (≥200 mg/dL).1
‡In the 6-week studies, the proportion of patients with shifts in fasting glucose from normal (<100 mg/dL) to high (≥126 mg/dL): VRAYLAR 1.5 mg/day + ADT=2%; VRAYLAR 3 mg/day + ADT=3.2%; placebo-treated=1.3%. The proportion of patients with shifts in fasting glucose from normal to borderline (≥100 and <126 mg/dL) or from borderline to high was similar in patients treated with VRAYLAR and placebo. In the 8-week study, the shifts in fasting glucose were similar among the VRAYLAR and placebo + ADT groups.1
§In two 6-week MDD studies, mean change from baseline in prolactin levels was 4.1 ng/mL and 3.8 ng/mL in the 1.5 mg/day + ADT group (baseline mean: 9.4 - 9.7) and 2.6 ng/mL and 2.9 ng/mL in the 3 mg/day group + ADT (baseline mean: 11.3 - 11.6) vs 1.2 ng/mL and 0.92 ng/mL in the placebo + ADT group (baseline mean: 9.7 - 10.5). In the 8-week MDD study, the mean change from baseline was 3.8 ng/mL in the 1-2 mg/day + ADT group (baseline mean: 8.8) and 4.1 ng/mL in the 2-4.5 mg/day + ADT group (baseline mean 9.4) vs 0.7 ng/mL in the placebo group (baseline mean: 9.4).2
| Placebo + ADT (n=503) | VRAYLAR 1.5 mg/day + ADT (n=502) | VRAYLAR 3 mg/day + ADT (n=503) | |
|---|---|---|---|
| Insomnia|| | 5% | 9% | 10% |
| Nausea | 3% | 7% | 6% |
| Akathisia¶ | 2% | 7% | 10% |
Most common adverse events in two trials that followed recommended titration.
Rates of somnolence and sedation in VRAYLAR 1.5 mg/day + ADT (5%) and 3 mg/day + ADT (6%) groups were similar to placebo + ADT (4%).2
||Insomnia terms: initial insomnia, insomnia, middle insomnia, poor sleep quality, sleep disorder, terminal insomnia.
¶Akathisia terms: akathisia, psychomotor hyperactivity, feeling jittery, nervousness, tension.
In two 6-week MDD studies, 4% of VRAYLAR-treated patients discontinued treatment compared with 2% of placebo-treated patients when following recommended titration schedule.
There were no adverse reactions leading to discontinuation that occurred at a rate of ≥2% in VRAYLAR patients and at least twice the rate of placebo.
| Placebo + ADT (n=503) | VRAYLAR 1.5 mg/day + ADT (n=502) | VRAYLAR 3 mg/day + ADT (n=503) | |
|---|---|---|---|
| Abnormal orgasm | 0% | 0% | 0.2% |
| Decreased libido | 0% | 0.2% | 0% |
| Erectile dysfunction | 0% | 0.2% | 0% |
| Ejaculation failure | 0% | 0.2% | 0% |
| Ejaculation disorder | 0% | 0% | 0% |
#These are self-reported adverse effects. If an adverse effect was not reported during a study, a value of 0 was used.
Well-established tolerability across weight and metabolics
Weight change ≤1.5 lb from baseline to endpoint in pivotal 6- and 8-week studies1*
| Mean change at endpoint | Proportion of patients with weight increase ≥7% | |
|---|---|---|
| Placebo (n=463) | -0.2 lb | 1% |
| VRAYLAR 1.5 mg/day (n=467) | +1.5 lb | 3% |
| VRAYLAR 3 mg/day (n=465) | +0.9 lb | 3% |
Placebo-like impact on lipids and fasting glucose from baseline to endpoint in pivotal studies1,2†
| Total cholesterol | Proportion of patients with metabolic shifts was similar to placebo |
|---|---|
| Fasting triglycerides | |
| Fasting glucose | |
| Prolactin (ng/mL) | No meaningful increase in mean levels |
(See adjunctive MDD tab above)
*Recommended dose range of VRAYLAR is 1.5–3 mg/day for depressive episodes associated with bipolar I.1
†Metabolic shift defined as: fasting glucose: normal (<100 mg/dL) to high (≥126 mg/dL), borderline (≥100 mg/dL and <126 mg/dL) to high; total cholesterol: normal/borderline (<240 mg/dL) to high (≥240 mg/dL); fasting triglycerides: normal/borderline (<200 mg/dL) to high (≥200 mg/dL).1,2
Well-established safety profile across 3 bipolar I depression studies
Most common adverse reactions (≥5% and at least twice that of placebo)1
| Recommended dose range | |||
|---|---|---|---|
| Placebo (n=468) | VRAYLAR 1.5 mg/day (n=470) | VRAYLAR 3 mg/day (n=469) | |
| Nausea | 3% | 7% | 7% |
| Akathisia | 2% | 6% | 10% |
| Restlessness | 3% | 2% | 7% |
| EPS‡ | 2% | 4% | 6% |
Rates of somnolence and sedation in VRAYLAR 1.5 mg/day (7%) and 3 mg/day (6%) groups were similar to placebo (4%)1
‡EPS included akinesia, drooling, dyskinesia, dystonia, extrapyramidal disorder, hypokinesia, muscle tightness, musculoskeletal stiffness, myoclonus, oculogyric crisis, salivary hypersecretion, tardive dyskinesia, and tremor.1
Discontinuation rates
Overall, 6% of the patients who received VRAYLAR discontinued treatment due to an adverse reaction, compared with 5% of placebo-treated patients in these trials1
§EPS excludes akathisia and restlessness.
Monitor patients when initiating or changing the dose of VRAYLAR1
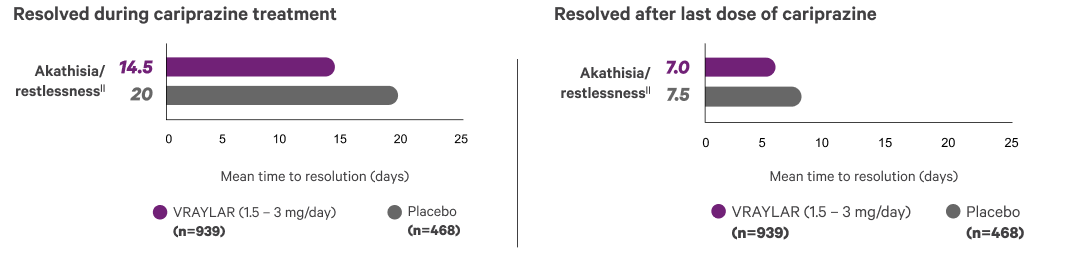
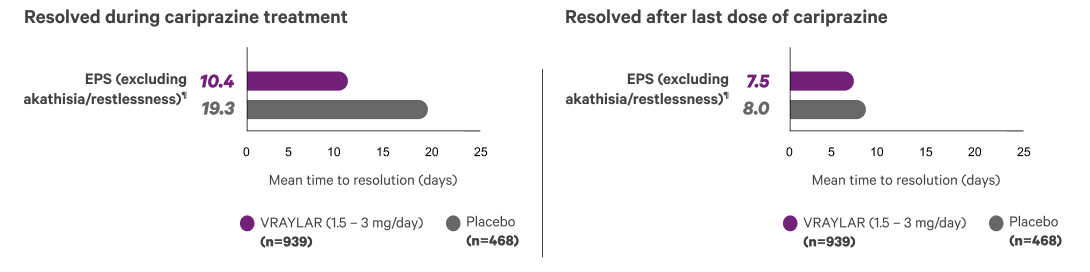
EPS and akathisia were among the most common adverse reactions and were most frequently observed following initiation or up-titration1,4
Sexual adverse reactions
Less than 1% of patients reported sexual adverse reactions across clinical studies2
| Most common reactions included: | |||
|---|---|---|---|
| Placebo (n=468) | VRAYLAR 1.5 mg/day (n=470) | VRAYLAR 3 mg/day (n=469) | |
| Abnormal orgasm | 0% | 0% | 0.4% |
| Decreased libido | 0% | 0.2% | 0% |
| Erectile dysfunction | 0% | 0.6% | 0.9% |
| Delayed ejaculation | 0% | 0% | 0% |
| Mean change at endpoint | Proportion of patients with weight increase ≥7% | |
|---|---|---|
| Placebo (n=439) | +0.4 lb | 2% |
| VRAYLAR 3-6 mg/day (n=259) | +1.1 lb | 1% |
Placebo-like impact on lipids and fasting glucose from baseline to endpoint in pivotal studies1,2†‡
| Total cholesterol | Proportion of patients with metabolic shifts was similar to placebo |
|---|---|
| Fasting triglycerides | |
| Fasting glucose | |
| Prolactin (ng/mL) | No meaningful increase in mean levels |
*Recommended dose range of VRAYLAR is 3–6 mg/day for manic and mixed episodes and 1.5–3 mg/day for depressive episodes associated with bipolar I. Doses above 6 mg daily did not appear to have additional benefit over lower doses and a dose-related increase in certain adverse reactions was observed.1
†Data shown from baseline to endpoint by modal daily dose, defined as most frequently administered dose per patient.1
‡Metabolic shift defined as: fasting glucose: normal (<100 mg/dL) to high (≥126 mg/dL), borderline (≥100 mg/dL and <126 mg/dL) to high total cholesterol: normal/borderline (<240 mg/dL) to high (≥240 mg/dL); fasting triglycerides: normal/borderline (<200 mg/dL) to high (≥200 mg/dL).1,2
| Recommended dose range | |||
|---|---|---|---|
| Placebo (n=442) | VRAYLAR 3-6 mg/day (n=263)§ | VRAYLAR 9-12 mg/day (n=360)§ | |
| EPSII | 12% | 26% | 29% |
| Akathisia | 5% | 20% | 21% |
| Vomiting | 4% | 10% | 8% |
| Dyspepsia | 4% | 7% | 9% |
| Somnolence¶ | 4% | 7% | 8% |
| Restlessness | 2% | 7% | 7% |
§Data shown from baseline to endpoint (Week 3) by modal daily dose, defined as most frequently administered dose per patient.1
IIEPS included bradykinesia, drooling, dyskinesia, dystonia, extrapyramidal disorder, hypokinesia, muscle rigidity, muscle tightness, musculoskeletal stiffness, oromandibular dystonia, parkinsonism, salivary hypersecretion, and tremor.1
¶Somnolence included hypersomnia, sedation, and somnolence.1
#EPS excludes akathisia and restlessness.
Monitor patients when initiating or changing the dose of VRAYLAR1
EPS and akathisia were among the most common adverse reactions and were most frequently observed following initiation or up‑titration1,6
| Mean change at endpoint | Proportion of patients with weight increase ≥7% | |
|---|---|---|
| Placebo (n=573) | +0.7 lb | 5% |
| VRAYLAR 1.5-3 mg/day (n=512) | +1.8 lb | 8% |
| VRAYLAR 4.5-6 mg/day (n=570) | +2.2 lb | 8% |
Placebo-like impact on lipids and fasting glucose from baseline to endpoint in pivotal studies1,2†‡
| Total cholesterol | Proportion of patients with metabolic shifts was similar to placebo |
|---|---|
| Fasting triglycerides | |
| Fasting glucose | |
| Prolactin (ng/mL) | No meaningful increase in mean levels |
*Recommended dose range of VRAYLAR is 1.5–6 mg/day for schizophrenia. Doses above 6 mg daily did not appear to have additional benefit over lower doses and a dose-related increase in certain adverse reactions was observed.1
†Data shown from baseline to endpoint (Week 6) by modal daily dose, defined as most frequently administered dose per patient.1,2
‡Metabolic shift defined as: fasting glucose: normal (<100 mg/dL) to high (≥126 mg/dL), borderline (≥100 mg/dL and <126 mg/dL) to high; total cholesterol: normal/borderline (<240 mg/dL) to high (≥240 mg/dL); fasting triglycerides: normal/borderline (<200 mg/dL) to high (≥200 mg/dL).1,2
Long-term maintenance treatment of schizophrenia in adults was assessed in a 92-week study of VRAYLAR1,7
Following a 20-week, open-label phase on a stable dose of VRAYLAR, patients were randomized to VRAYLAR 3-9 mg/day or placebo for a 72-week, double-blind phase.1,7
| 72-week, double-blind phase | ||
|---|---|---|
| Placebo (n=99) | VRAYLAR 3-9 mg/day (n=101) | |
| Weight change (lb)§ | +2.1 | +2.5 |
| Fasting glucose (mg/dL) | +4.1 | +5.4 |
| Fasting triglycerides (mg/dL) | -7.6 | +2.8 |
| Total cholesterol (mg/dL) | -6.5 | -4.1 |
| Prolactin (ng/mL) | -6.4 | -6.7 |
Recommended dose range of VRAYLAR is 1.5-6 mg/day. Doses above 6 mg daily did not appear to have additional benefit over lower doses, and a dose-related increase in certain adverse reactions was observed.
§Proportion of patients with weight gain ≥7% was 10.6% during the open-label phase and 27.0% and 32.3% for VRAYLAR and placebo-treated patients, respectively, during the double-blind phase.7
| Recommended dose range | |||||
|---|---|---|---|---|---|
| Placebo (n=584) | VRAYLAR 1.5-3 mg/day (n=539)II | VRAYLAR 4.5-6 mg/day (n=575)II | VRAYLAR 9-12 mg/day (n=203)II | ||
| EPS¶ | 8% | 15% | 19% | 20% | |
| Akathisia | 4% | 9% | 13% | 14% | |
IIData shown from baseline to endpoint (Week 6) by modal daily dose, defined as most frequently administered dose per patient.1,2
¶EPS included bradykinesia, cogwheel rigidity, drooling, dyskinesia, dystonia, extrapyramidal disorder, hypokinesia, masked facies, muscle rigidity, muscle tightness, musculoskeletal stiffness, oculogyric crisis, oromandibular dystonia, parkinsonism, salivary hypersecretion, tardive dyskinesia, torticollis, tremor, and trismus.1
Overall, 9% of the patients who received VRAYLAR discontinued treatment due to an adverse reaction, compared with 12% of placebo-treated patients in these trials
These data include patients who discontinued due to worsening of schizophrenia (ie, untreated illness).
#EPS excludes akathisia and restlessness.
Monitor patients when initiating or changing the dose of VRAYLAR1
EPS and akathisia were among the most common adverse reactions and were most frequently observed following initiation or up‑titration1,8
ADT=antidepressant therapy; BP-I=bipolar I disorder; DSM=Diagnostic and Statistical Manual of Mental Disorders; EPS=extrapyramidal symptoms; MDD=major depressive disorder.
VRAYLAR (cariprazine) is indicated in adults as adjunctive therapy to antidepressants for the treatment of major depressive disorder (MDD), for the treatment of depressive episodes associated with bipolar I disorder (bipolar depression), for the acute treatment of manic or mixed episodes associated with bipolar I disorder, and for the treatment of schizophrenia.
WARNINGS: INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS and SUICIDAL THOUGHTS AND BEHAVIORS
Contraindication: VRAYLAR is contraindicated in patients with known hypersensitivity. Reactions have included rash, pruritus, urticaria, and reactions suggestive of angioedema.
Cerebrovascular Adverse Reactions, Including Stroke: In clinical trials with antipsychotic drugs, elderly patients with dementia had a higher incidence of cerebrovascular adverse reactions, including fatalities, vs placebo. VRAYLAR is not approved for the treatment of patients with dementia-related psychosis.
Neuroleptic Malignant Syndrome (NMS): NMS, a potentially fatal symptom complex, has been reported with antipsychotic drugs. NMS may cause hyperpyrexia, muscle rigidity, delirium, and autonomic instability. Additional signs may include elevated creatine phosphokinase, myoglobinuria (rhabdomyolysis), and acute renal failure. Manage with immediate discontinuation, intensive symptomatic treatment, and monitoring.
Tardive Dyskinesia (TD): Risk of developing TD (a syndrome of potentially irreversible, involuntary, dyskinetic movements) and the likelihood it will become irreversible may increase with the duration of treatment and the cumulative dose. The syndrome can develop after a relatively brief treatment period, even at low doses, or after treatment discontinuation. If signs and symptoms of TD appear, drug discontinuation should be considered.
Late-Occurring Adverse Reactions: Adverse reactions may first appear several weeks after initiation of VRAYLAR, probably because plasma levels of cariprazine and its major metabolites accumulate over time. As a result, the incidence of adverse reactions in short-term trials may not reflect the rates after longer-term exposures. Monitor for adverse reactions, including extrapyramidal symptoms (EPS) or akathisia, and patient response for several weeks after starting VRAYLAR and after each dosage increase. Consider reducing the dose or discontinuing the drug.
Metabolic Changes: Atypical antipsychotics, including VRAYLAR, have caused metabolic changes, such as:
Leukopenia, Neutropenia, and Agranulocytosis: Leukopenia/neutropenia have been reported with antipsychotics, including VRAYLAR. Agranulocytosis (including fatal cases) has been reported with other antipsychotics. Monitor complete blood count in patients with pre-existing low white blood cell count (WBC)/absolute neutrophil count or history of drug-induced leukopenia/neutropenia. Discontinue VRAYLAR at the first sign of a clinically significant decline in WBC and in severely neutropenic patients.
Orthostatic Hypotension and Syncope: Atypical antipsychotics cause orthostatic hypotension and syncope, with the greatest risk during initial titration and with dose increases. Monitor orthostatic vital signs in patients predisposed to hypotension and in those with cardiovascular/cerebrovascular diseases.
Falls: VRAYLAR may cause somnolence, postural hypotension, motor and sensory instability, which may lead to falls and, consequently, fractures or other injuries. For patients with diseases, conditions, or medications that could exacerbate these effects, complete fall risk assessments when initiating antipsychotics and recurrently for patients on long-term therapy.
Seizures: Use VRAYLAR with caution in patients with a history of seizures or with conditions that lower the seizure threshold.
Potential for Cognitive and Motor Impairment: Somnolence was reported with VRAYLAR. Caution patients about performing activities requiring mental alertness (eg, operating hazardous machinery or a motor vehicle).
Body Temperature Dysregulation: Use VRAYLAR with caution in patients who may experience conditions that increase body temperature (eg, strenuous exercise, extreme heat, dehydration, or concomitant anticholinergics).
Dysphagia: Esophageal dysmotility and aspiration have been associated with antipsychotics. Antipsychotic drugs, including VRAYLAR, should be used cautiously in patients at risk for aspiration.
Drug Interactions: Strong and moderate CYP3A4 inhibitors increase VRAYLAR concentrations, so VRAYLAR dose reduction is recommended. Concomitant use with CYP3A4 inducers is not recommended.
Adverse Reactions: The most common adverse reactions in clinical trials (≥5% and at least twice the rate of placebo) are listed below:
US-VRA-240286
References: